The endocrine system is a critical component of our physiology. In other words, it is the system that produces hormones that regulate many of our body’s activity, so for example, the thyroid produces thyroid hormone which controls our metabolism our heart our resting heart rate our basal metabolic rate and so it can control things like our metabolism and weight for example.
The parathyroid glands are actually small right next to the thyroid, and hence their name parathyroid they are responsible for controlling the calcium levels in our body calcium is an essential element for all sorts of important physiologic processes, including heart and muscle contraction nerve impulses for thinking and movement.
The adrenal glands are similarly important; they are responsible for producing a variety of hormones including adrenaline, cortisol and mineralocorticoids which help regulate our basic physiology and fluid balance.
As far as risk factors for endocrine tumor problems, it should be understood that the vast majority of these tumors occur in people without risk factors that being said there are several family syndromes in which thyroid and parathyroid tumors are an important component the multiple endocrine neoplasia syndromes are a classic example of this but by and large there as far as the tumors or surgical disorders of the endocrine system there are fairly few risk factors.
The one big exception being exposure to radiation therapy but that is more of a consideration in the past as we don’t as we no longer at least for therapeutic reasons use sufficient doses of radiation to cause problems to the thyroid.
Consultation with an endocrine surgeon has indicated in a variety of circumstances the presence of a thyroid nodule is certainly a good reason to see an endocrine surgeon even though the vast majority of patients do not need surgery however the evaluation and management certainly fall within the expertise of the endocrine surgeon.
Our research laboratory is actively involved in understanding the pathogenesis and outcomes of patients with hyperparathyroidism. The mechanisms of abnormal calcium sensing by parathyroid tumors and important discoveries in the growth and function of these tumors.
I think it is very important that surgeons who are engaged in the clinical care of patients with endocrine disorders be actively involved in research in this area. There’s a considerable advantage to having the expertise brought about not only by the clinical practice of endocrine surgery but also by understanding the disorder’s basic tumor biology and biology.
Starting with diabetes, we know that patients with diabetes have increased perioperative morbidity and mortality compared to patients without diabetes who are undergoing those same surgeries. .
It’s been shown that perioperative glucose levels on the surgical date and those first few postoperative days correlate with perioperative complications more strongly than preoperative hemoglobin A1C levels. The target glucose range is 80 to 180 milligrams per deciliter.
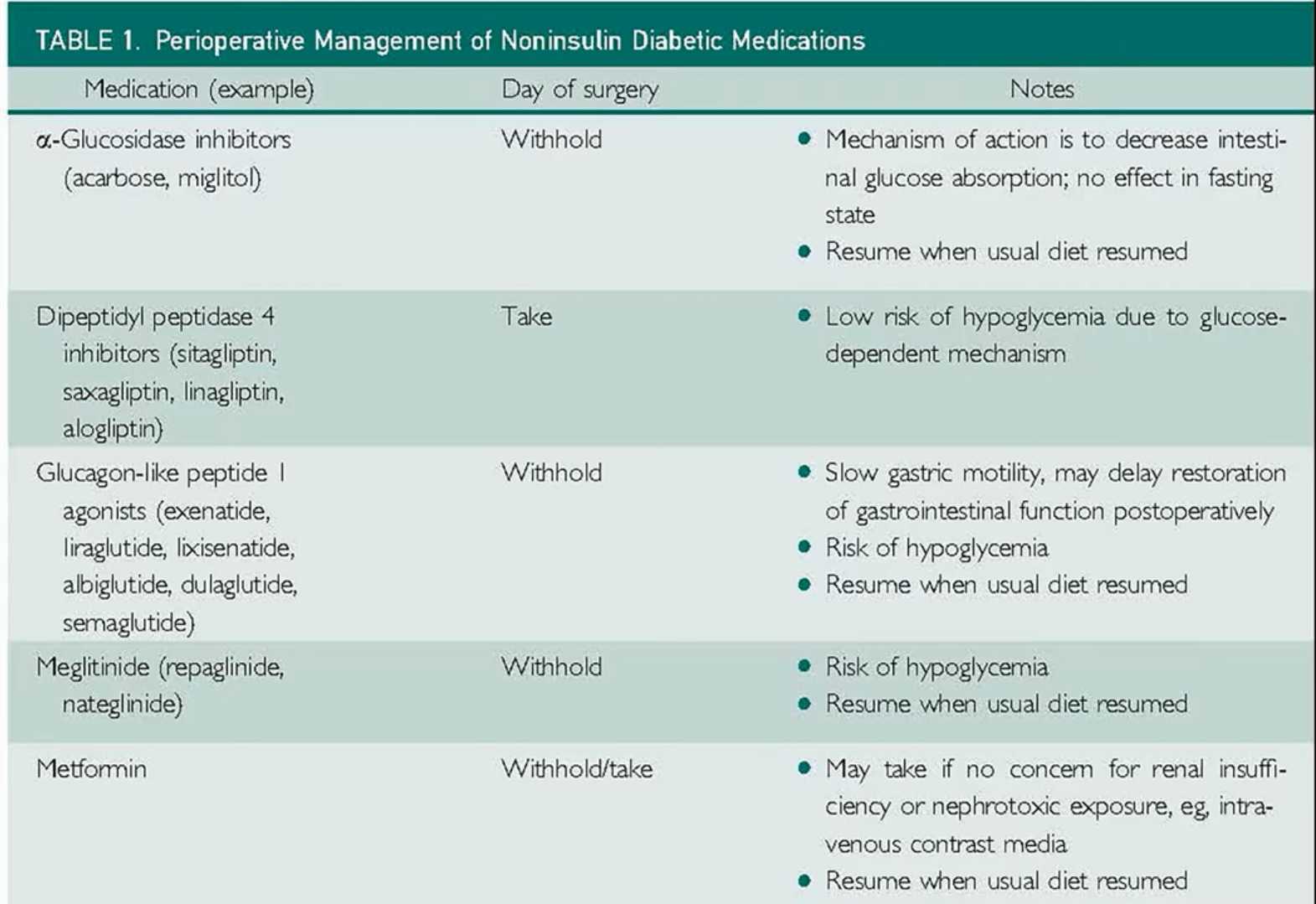
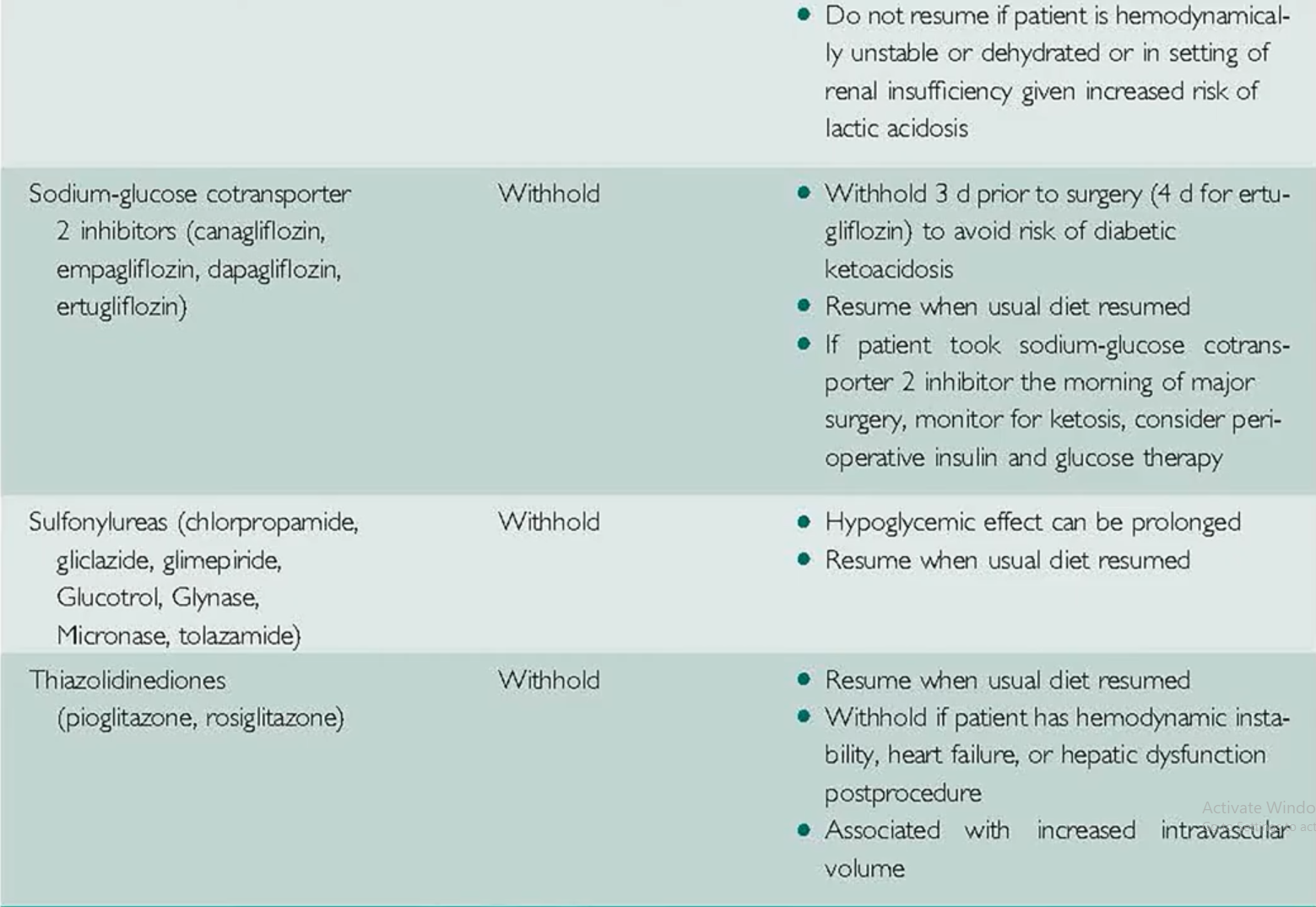
Tighter glycemic control is not associated with better outcomes in these patients but is associated with increased rates of hypoglycemia. As far as medication recommendations, non-insulin diabetic medications should be held the morning of surgery and typically restarted once the patient is eating normally. The main exception to this is the SGLT2 inhibitors which should be held for three days before surgery, and this is to avoid the rare complication of diabetic ketoacidosis.
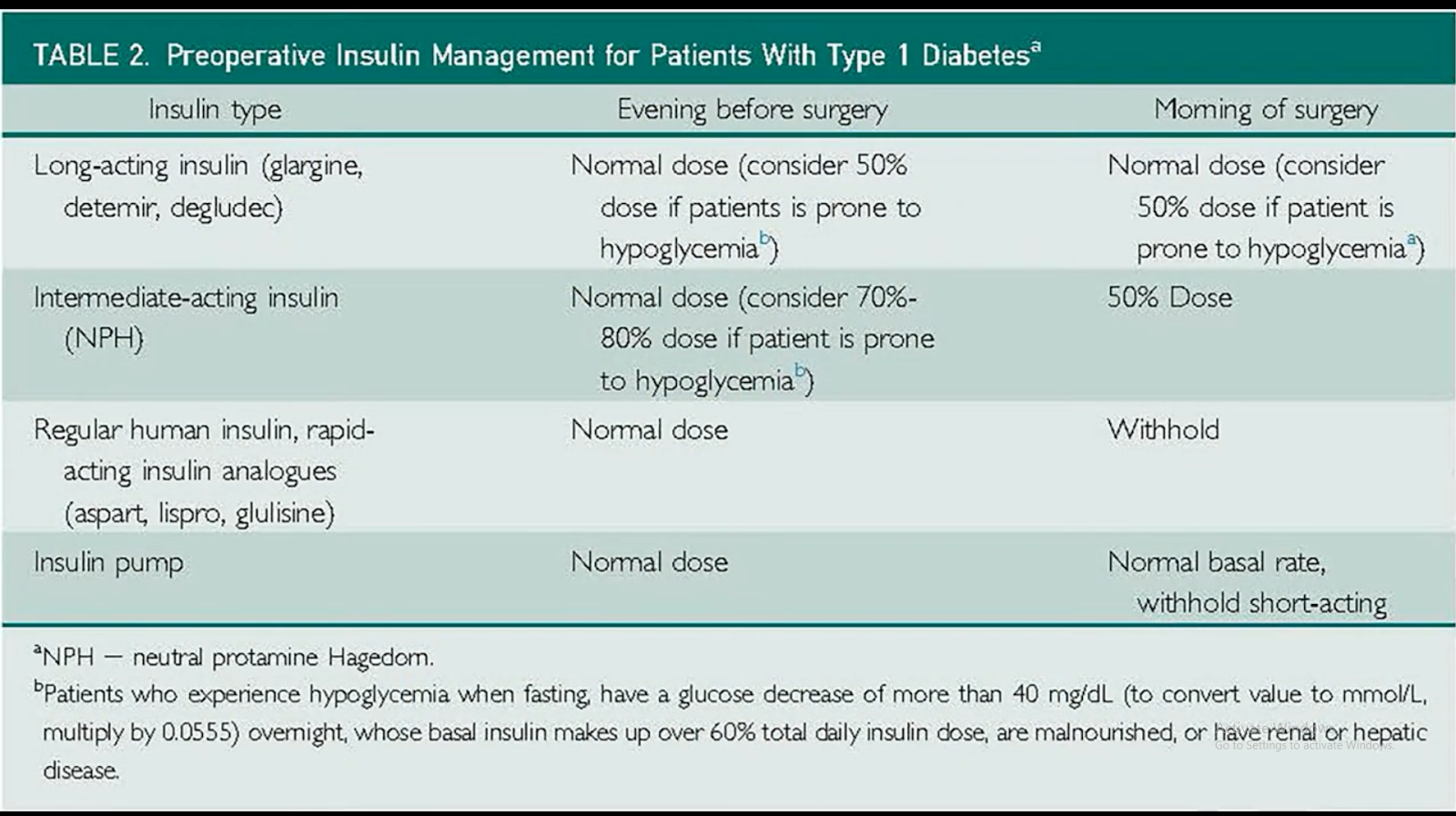
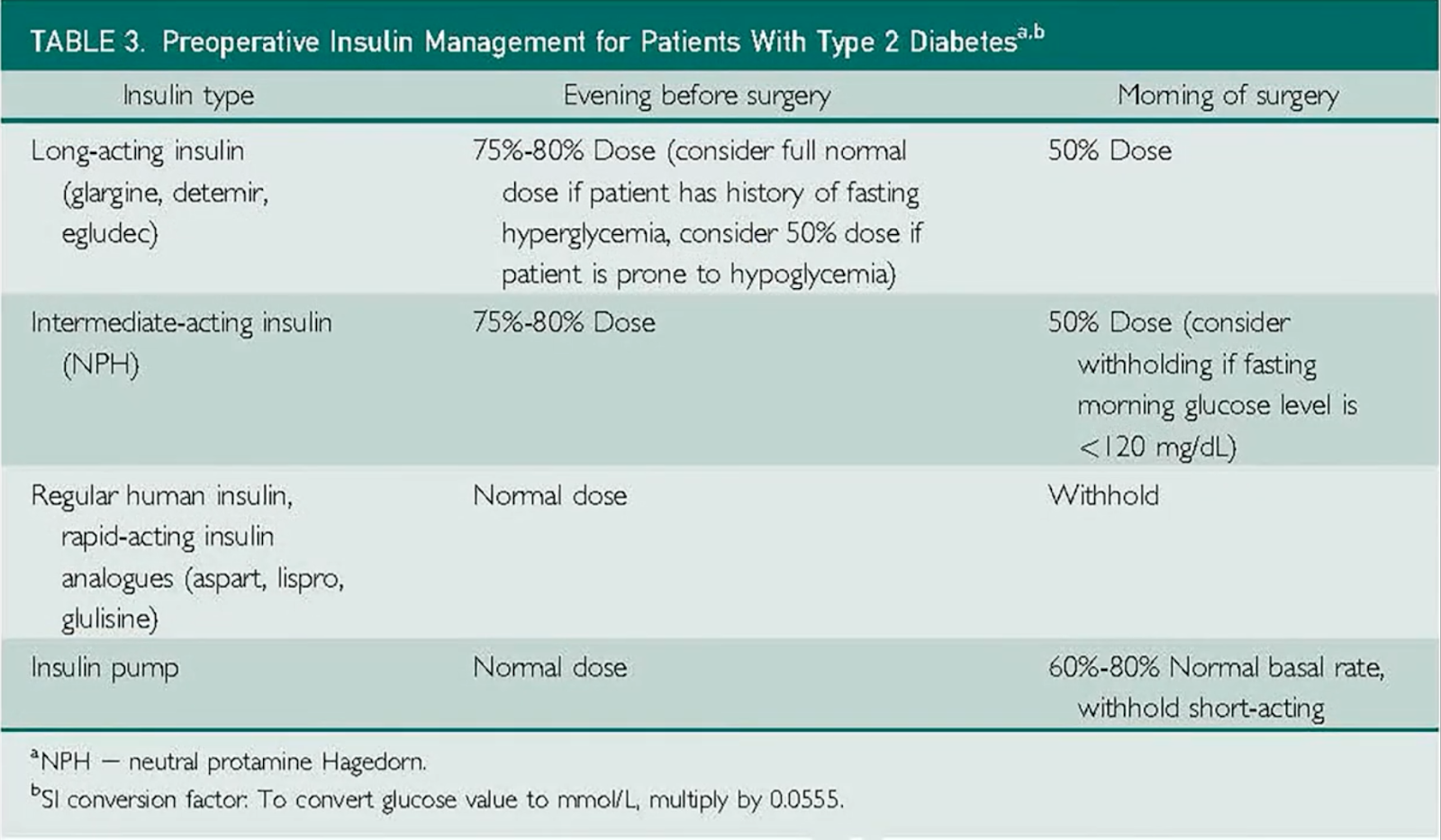
Recommendations for preoperative insulin differ based on diabetes, the type of insulin, and the patient’s predisposition to hypo or hyperglycemia. Tables two and three of the review break this down for you and give insulin dosing recommendations for the day before and the day of surgery.
Now moving on to patients with thyroid disease, patients with subclinical hypothyroidism or mildly reduced free thyroxine levels don’t have increased perioperative risk. Therefore, it is safe to proceed with surgery.
On the other hand, patients with severe hypothyroidism and particularly patients with myxedema coma are at very high risk for perioperative cardiac and pulmonary complications. Therefore, surgery should be deferred if urgent or emergent surgery is needed in these patients started on iv thyroid hormone replacement right away.
Now for patients with hyperthyroidism, it is recommended that elective surgeries be deferred until the patient is thyroid. For urgent or emergent surgeries, these patients should be pre-treated with beta-blockade antithyroid agents and corticosteroids.
So finally, which patients should receive perioperative stress dose steroids? Again, this is a controversial topic, and the evidence has very limited the need for stress dose steroids is determined by the invasiveness of the procedure, the dose and duration of steroid exposure, and testing of the hypothalamic-pituitary-adrenal access if needed.
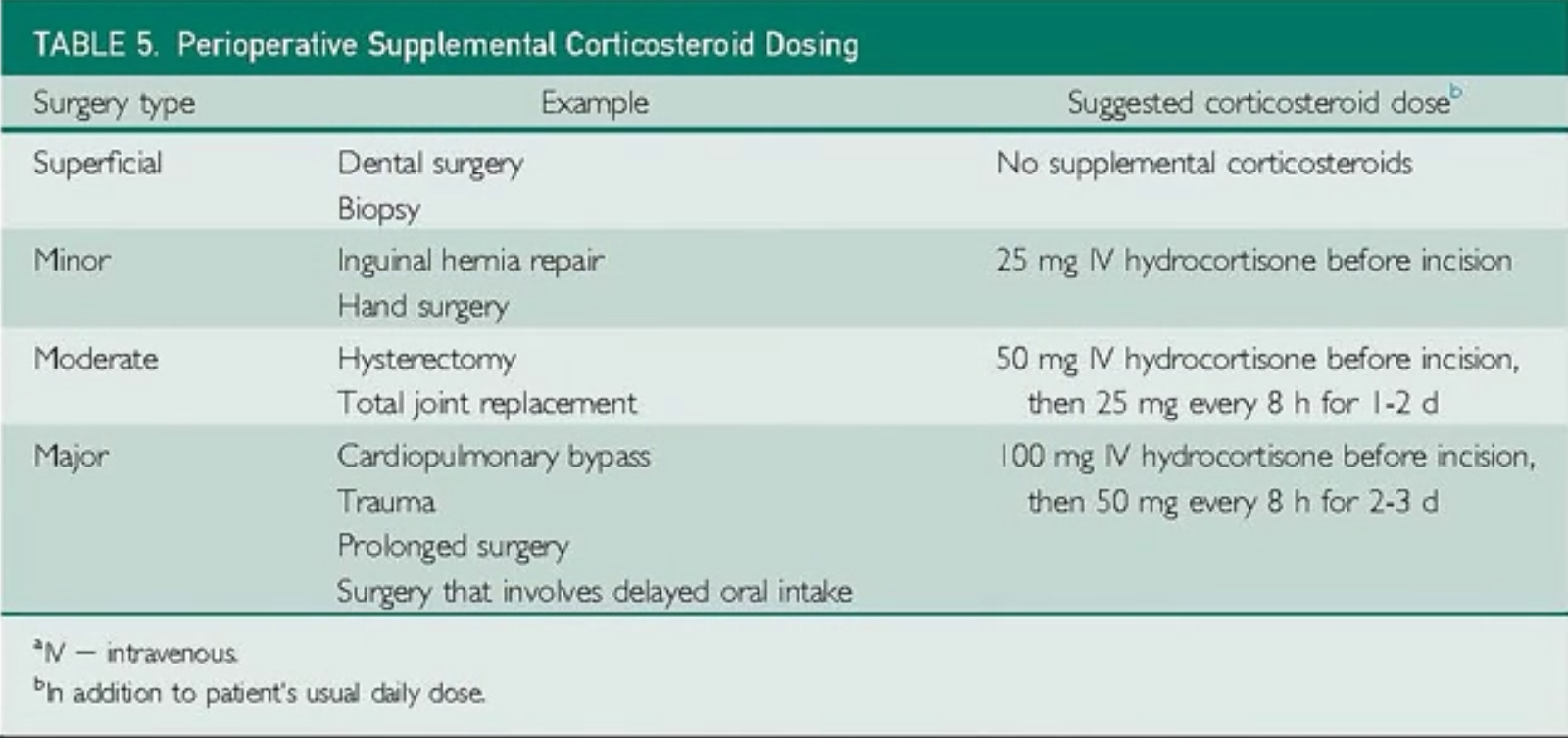
Giving supplemental steroids to all patients with known adrenal insufficiency and also all patients who have been on doses greater than or equal to five milligrams of prednisone daily for over three weeks within the past three months and also patients on high dose inhaled corticosteroid therapy,
So, in summary, surgical patients with endocrine issues require special consideration in the perioperative period for diabetes. Remember, the most important thing for these patients is ensuring that they remain in that target glucose range in the perioperative period for thyroid disease. Surgical plans only need to be altered if the patient has hyperthyroidism or severe hypothyroidism. The evidence for stress dose steroids is very limited but for specific patient populations with chronic steroid exposure.